Arthrofibrosis is a serious condition that can afflict knee joints that have either been recently injured, operated upon, or both. The process begins when the traumatic stimulus of an injury and/or surgery leads the knee to form extensive, internal scar tissue. This is followed by shrinkage and tightening of the knee's joint capsule (surrounding envelope ligament). Sometimes even nearby tendons outside of the joint stiffen up. This internal and external tightening process may continue to the point where motion between the femur (thigh bone) and tibia (shin bone) is severely restricted. Afflicted patients may permanently lose the ability to fully straighten and/or bend their knee. In general, the likelihood of developing arthrofibrosis increases with the severity of a knee joint injury, the extensiveness of related surgery, and the length of time that the knee is subsequently immobilized. However, not everyone who sustains a major knee injury or who undergoes major surgery will develop arthrofibrosis. Some people are more prone to developing this problem than others. Genetic factors apparently predispose some patients to develop arthrofibrosis by way of an inherited tendency to form hypertrophic (excessive) internal joint scar tissue in response to injury and/or surgery. Such individuals often heal surgical ligament repairs and grafts quite solidly, but go on to heal "excessively", forming an overabundance of unwanted fibrous scar in their knee. This essentially makes their knee too stable, to the point of being stiff and lacking proper joint motion. Such "heavy scar-formers" can literally fill up their entire knee joint cavity with thick, tough scar tissue. This obliterates all of the normal open spaces within the joint, adhering everything together and effectively "freezing" the joint (hence the traditional term "frozen joint"). Patients with "sensitive" knees or low pain thresholds are also more likely to develop this problem, as they find it more difficult than most to use and move their knee after injury or surgery. Lack of joint motion and use leads the knee to form more abundant and less compliant scar tissue than it otherwise would, and allows the relatively unused (and thus unstretched) surrounding knee capsule to contract down and tighten up, almost like "shrink-wrap" does. A stiff, arthrofibrotic knee is a very difficult problem for the orthopedic surgeon and physical therapist to handle. It usually requires a specially planned, intensive protocol of surgical treatment and post-operative management. The traditional treatment approach for arthrofibrotic knees that did
not loosen up with aggressive stretching and exercise in physical therapy
has been to place the patient under anesthesia and then literally break
up and tear the restrictive, internal scar tissue within the joint by
forcing the knee to fully bend and straighten. The surgeon accomplishes
this by way of strenuous, manual joint manipulation. The procedure therefore
came to be known as a manipulation under anesthesia, or "M.U.A.",
and is still in common use. In cases of severely frozen knees, extremely
stressful manipulation forces may be required to break up the scar tissue
and get the joint moving again. This poses a risk to a patient who has
not been able to bear much weight on their leg for quite some time,
because the femur and tibia may have lost a considerable amount of bone
mineral (calcium phosphate), thus weakening them. This increases the
chance of an inadvertent femoral or tibial fracture occurring
at the time of the joint manipulation. My preference over the years
has been to perform an arthroscopic, internal surgical scar resection
to remove as much restrictive scar tissue as possible, prior
to manipulating the knee. This approach not only leaves very little
scar within the joint to re-organize and solidify once again, but it
also reduces the manipulation force required to get the knee moving,
thus reducing (but not eliminating) the chance of femoral or tibial
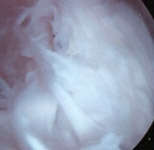
fracture. Surgical TreatmentThe procedure of arthroscopically removing internal knee joint scar is often long and tedious. Sometimes the joint is packed so thickly with scar tissue that removing it is akin to a slow, meticulous archeological excavation process. The normal internal joint anatomy must be carefully exposed, millimeter by millimeter, as the scar tissue is gradually cut away and removed. All of the internal joint spaces that are normally present should be opened up and restored in this fashion prior to attempting knee manipulation (see FIGURES 1a, 1b, 1c). The lateral retinaculum (capsular envelope ligament just to the outer side of the kneecap) is often especially contracted and tight, and usually must be surgically released (divided) at the same time.
In severe cases where the posterior (rear) capsule of the knee is
also tightly contracted, thus restricting full knee extension (straightening)
despite attempted knee manipulation, an open (non-arthroscopic)
posterior capsular surgical release may be required. A technique using
a small lateral knee incision may be utilized to minimize surgical dissection
trauma directly behind the knee as well as skin scarring. Post-Operative CareNo matter how meticulous and thorough a scar tissue resection may be, and even if a full range of knee motion is successfully restored on the operating room table, the biggest challenge is maintaining that range of motion after surgery. New scar tissue may rapidly re-form within the joint unless comprehensive action is taken to avoid this. Unless special post-operative pain relief measures are taken, attempting to move the joint through its full range of motion immediately after surgery may simply be intolerable. Unfortunately, if the patient does not move their knee through a full arc of motion repeatedly and fairly continuously in the first 2 to 3 post-operative weeks, they are at risk of having their knee joint become "frozen" once again. Aside from knees where only joint extension is lacking (which are often best held in a maximally extended position in a full-leg cast for the first several post-op days), the key to better results following surgical procedures for arthrofibrosis is to perform them under epidural anesthesia and to maintain this or a supplemental regional, pain-relieving, anesthetic nerve block for a day or two post-operatively, so as to allow joint motion without the inhibiting effect of severe pain. I have been using this anesthetic method following arthrofibrosis surgery for well over a decade. Taking advantage of the ongoing pain relief afforded by the extended anesthetic block effect, a program of immediate post-operative physical therapy is begun and continued, utilizing special, passive stretching techniques at the extremes of the knee's range of motion. The patient is also taught how to do their own stretching therapy, to supplement their supervised treatment. A continuous passive joint motion (CPM) machine is used in between stretching sessions, beginning in the recovery room and then continuing at home. This device is a mechanical leg cradle that gently bends and straightens the knee while the patient is lying down in bed. Post-operative medication to inhibit recurrent fibrous scar tissue formation within the knee is also often helpful. Possibilities include intra-articular (injected into the joint) hyaluronate (a joint lubricant) and/or corticosteroid (cortisone) medication administered on one or more occasions in the first post-operative month or two. Faithful patient compliance with prescribed outpatient physical therapy treatment and diligent, self-administered stretching in the post-operative phase is critical. Supplemental treatment with an oral anti-inflammatory medication (if the patient's stomach can tolerate it) is helpful. A severe case of arthrofibrosis can be an extremely difficult challenge for both patient and knee surgeon alike. In this author's experience, the comprehensive treatment program described above has met with good results in most circumstances, including cases of total knee joint replacement that still demonstrated a restricted range of motion despite one or more attempts at manipulation under anesthesia without arthroscopic intervention.
|
|||||||||||||||||||||||||||