
|
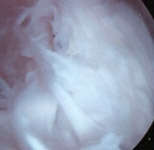 |
FIGURE 1a -Arthroscopic view during an early stage of a scar resection procedure in a patient with severe knee arthrofibrosis. This patient's entire internal joint space was filled up with tough, fibrous scar tissue (the white, fluffy/fibrous material seen in this photo), which is nearly all that can be seen here! An arthroscopic tissue resector instrument has removed some scar already, creating a small, open "working space", which is where the lens of the arthroscope was situated when this picture was taken. The resector is then used to progressively remove more and more scar tissue, gradually enlarging the working space, until an anatomic landmark (such as one of the femoral condyles) is uncovered. |
 |
FIGURE 1b - Arthroscopic view of the same patient's knee, but further along in the procedure. In the background you can see that the arthroscopic scar resector (shiny metal object to the left) has uncovered a portion of the smooth, white femoral condylar surface, marked with an "F". Once such a landmark is identified, the surgeon can then more safely and effectively "excavate" the rest of the knee joint's anatomy out from the mass of scar tissue that has engulfed it. The goal is to open up all of the internal joint spaces to normal or near-normal dimensions, fully exposing the normally free and unencumbered intra-articular joint structures. |
 |
FIGURE 1c - Arthroscopic view of the same patient's medial joint compartment at the conclusion of the case. The normal, internal joint space has been restored and the medial femoral condyle has been completely released from its enveloping scar tissue cocoon. Similar work has also been done in other knee compartments, in combination with a retinacular release. At this point, the knee is tested to see what free range of motion it has, and if necessary, joint manipulation and stretching are performed to restore the range of motion to normal. With almost all of the internal scar tissue that was formerly restricting the joint removed, the joint manipulation procedure will require significantly less applied force to regain the same range of motion, thus reducing the chance of an inadvertent femoral or tibial fracture. |
In severe cases where the posterior (rear) capsule of the knee
is also tightly contracted, thus restricting full knee extension
(straightening) despite attempted knee manipulation,
an open (non-arthroscopic) posterior capsular surgical release
may be required. A technique using a small lateral knee incision
may be utilized to minimize surgical dissection trauma directly
behind the knee as well as skin scarring.
|
|
|
|
|
|